|
Eyelid surgery by unlicensed practitioners:
complications and management
by Prof Dr Chua Chung Nen
Case 1

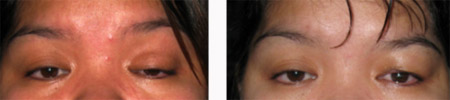
A 25 year-old woman complained of bilateral low skin
creases 12 months after Asian blepharoplasty (picture on the right).
The surgery was performed in a hotel by an unlicensed doctor from
oversea using the suture technique. She was unhappy with the
appearance and returned to the doctor asking for the skin creases to
be raised. However, she was informed that further surgery was not
possible. Her ocular examination was normal and the skin creases
measured 5 mm with some overhanging of skin over the creases. After
discussing with the patient, a revisional double eyelid surgery was
performed and the skin creases were raised to 7mm (picture on the
left).
Case 2

A 50 year-old woman presented with bilateral ptosis and
asymmetrical skin creases. She underwent Asian blepharoplasty in a
hair salon two years ago. Suture technique was employed. She returned
to the beautician for correction but was told that her eyes were
normal. She required revisional surgery to lower the left skin crease
and to lift the eyelid via levator resection.
Case 3

A 15 year-old girl presented with multiple swellings of
both upper eyelids along the skin creases. She underwent four Asian
blepharoplasties over the past 12 months. The procedures were
performed by the same beautician in a hair salon over a two year
period. However, the skin creases failed to form adequately and after
the last surgery which was 9 months ago, she was left with unsightly
lumps in her upper eyelids. The beautician was unable to offer any
remedial treatment for the swellings. To resolve the problem, she
underwent an incisional method of Asian blepharoplasty to remove the
swellings and to create new skin creases. Intraoperatively, the lumpy
lesions were found to be caused by prolene sutures. These sutures were
excised and skin creases were created with a height of 7 mm. She made
an uneventful recovery.
Case 4
A 35 year-old woman presented with a left congenital
ptosis. The left eye had poor levator function measuring only 3 mm and
the left upper skin crease was poorly formed. She consulted a
beautician one year ago and was advised to have a left Asian
blepharoplasty as the beautician assumed that the ptosis was caused by
the absence of the left upper eyelid skin crease. Following a suture
technique to create a left skin crease, the ptosis failed to improve
and the left skin crease was poorly formed. She returned to the
beautician but was informed that no further surgery was possible. We
performed a left frontalis suspension procedure using the pentagon
configuration with 2/0 prolene suture and the ptosis was
satisfactorily corrected. |
